First 1000 Days & Double Burden of Malnutrition
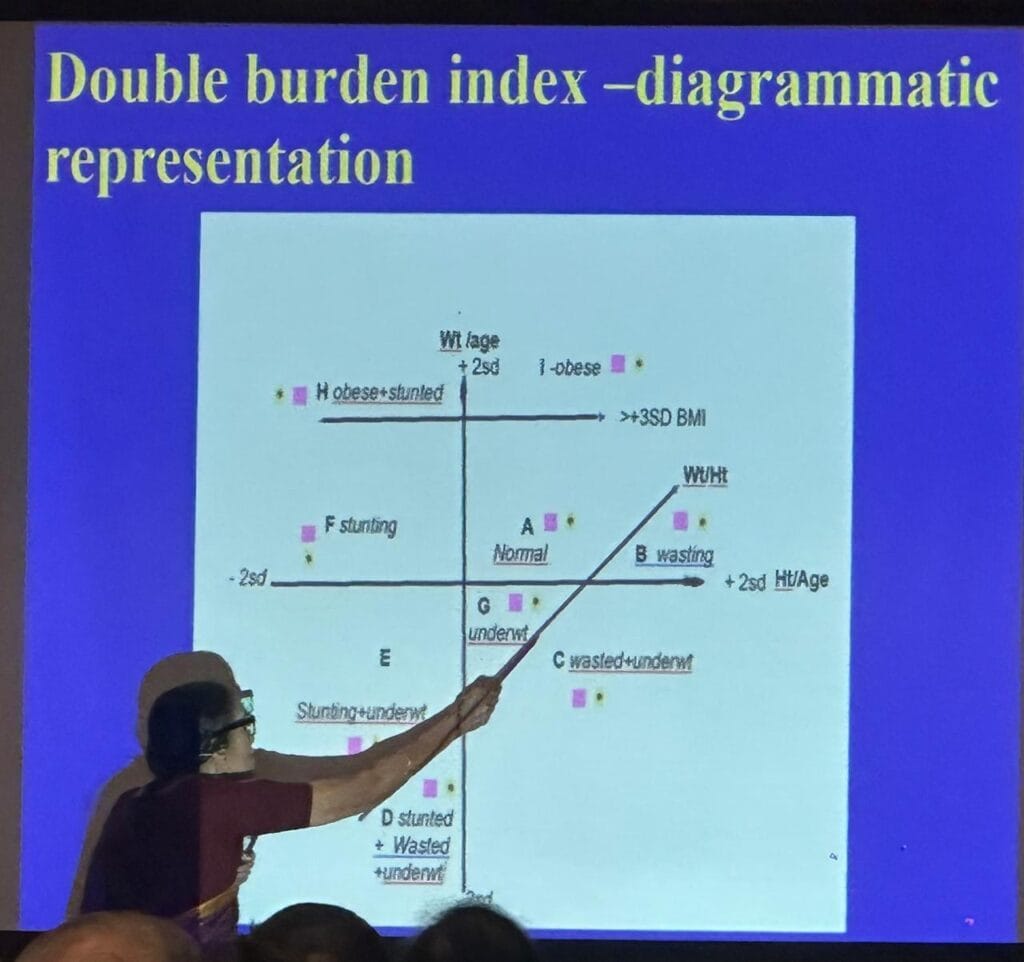
First 1000 Days & Double Burden of MalnutritionWhat I learnt in workshop (UNICEF, IAP) at Mumbai.In OPD and in the community, we often see: 1) large mother with small child, 2) small mother with large child, 3) a small infant becoming overweight in school age, 4) one small child and another large child of the same mother. We notice this. We wonder… and then we leave it at that. We rarely ask — why has this disparity occurred? We should, in fact, find out why and institute remedial measures. That is our job. Same house. Same kitchen. Same mother. But different nutritional outcomes.Children: undernutrition, overnutrition.Mother: undernutrition, overnutrition. This is not a food quantity problem. It is a nutrition quality problem. A behaviour problem. Acaregiver ecosystem problem. It is not enough to say, “Child is underweight, give more food…”or “Child is overweight, give less food…” Instead, we need to understand how the family eats.Because this family is not suffering from lack of food. They are suffering from lack of direction.This is the double burden of malnutrition (DBM) — right in front of us. We already knew a great deal. Malnutrition, undernutrition, overnutrition, marasmus,kwashiorkor, PCM, PEM, PJM (joules), SAM, MAM, ecology of malnutrition, growth, growthcurves, growth monitoring, anthropometry, anthropometric indices, percentile charts, ICMR,IAP, NCHS, WHO, hidden hunger, micronutrient deficiencies. Our understanding has beenevolving over decades. The Mumbai workshop gave a newer and better point of view. Nutritional assessment througha life-course approach — from intrauterine life to adulthood. A standardized, easy to understand and easy to use tool, the Double Burden Index (DBI), forassessing and classifying nutritional status across ages, situations, and purposes. DBI is forseeing today’s nutrition, understanding the past, and anticipating the future. Because nutritionis not a moment. It is a journey. Double burden of malnutrition (DBM) refers to the coexistence of undernutrition andovernutrition within the same individual, household, or community. One person can experienceboth undernutrition and overnutrition in the same life. One family can have both at the sametime. One community can have both at the same time. We learnt the importance of time in nutrition. Undernutrition during the foetal period and earlychildhood is common. It leads to biological adaptations — metabolic programming, anadjustment to scarcity. This is followed by excess or imbalanced nutrition later in life. The resultis a metabolic mismatch. It increases the risk of non-communicable diseases. What protects thefoetus in scarcity may harm the adult in abundance. The Double Burden Index (DBI) is a visual tool. Children cannot be only either undernourishedor overnourished. Multiple forms of malnutrition may coexist within the same child across time.This shifts clinical thinking from a static to a dynamic, longitudinal perspective. We have to think beyond nutritional interventions. Addressing only undernutrition or onlyobesity is insufficient. We have to consider the life cycle — from maternal health to earlychildhood and beyond. From a clinical and public health point of view, DBI encourages pediatricians to look beyondsymptoms and signs and assess the nutritional history and context of the child. It suggestsstrengthening the caregiver ecosystem. Families and communities need to be informed in alanguage they understand. We must understand the DBI chart and how to use it — to see the problem, not just understandit. This chart shows that the child is not just undernourished or overnourished. The same child canbe both. On this graph, we are not plotting numbers. We are plotting real children we see everyday in OPD. The horizontal axis represents BMI, from thin to obese. The vertical axis represents height forage, from stunted to normal or tall. Every point on this graph is a child with a story. At the center is the child we all want — normal height and normal weight. In the lower right arewasted children, thin for height, representing acute undernutrition. In the lower left arestunted children, short for age, representing chronic undernutrition. In the upper right areoverweight children, who may appear healthy but are metabolically at risk. In the upper left isthe double burden child — short but overweight. Undernourished in early life, overnourishedlater. Biology confused, metabolism strained. We have all seen this. A large mother with a small child, a small mother with a large child, ortwo siblings — one thin and one obese. But we rarely stop to ask why. This framework providesthe answer. Double burden is not two separate problems. It is one life-course problem. Early undernutritionleads to stunting. Later excess leads to obesity. The result is a high-risk phenotype. The body isprogrammed for scarcity but is forced to live in abundance. This reflects Barker’s hypothesis. Earlier we used to ask — is the child undernourished or overnourished? Now we must ask —how many forms of malnutrition exist in this same child? So when we see a child, we are not seeing today’s nutrition. We are seeing the history ofnutrition. Malnutrition is not only a medical problem. It is also a social problem. The pediatrician’s rolemust expand from clinical care to community engagement, caregiver education, and knowledgetransfer. In summary, the most important shift is from viewing malnutrition as a single condition tounderstanding it as a continuum shaped by time, environment, and biology. This perspectivehas significant implications for both clinical practice and program design. – Dr. Anil Mokashi (Pediatrician)MBBS, MD, DCH, FIAP, PhD(Child Growth and Development)

